Common Heart Tests Explained: What to Expect

Common heart tests explained in a clear, accessible way — understanding what each cardiac diagnostic test does, why it is ordered, and what its findings mean — helps patients engage meaningfully with their cardiovascular care. Cardiac diagnostic testing has advanced remarkably in the past two decades: tests that once required catheterization or hospitalization can now be performed non-invasively in 20 to 60 minutes, providing cardiologists with detailed information about the heart’s electrical activity, mechanical function, valve integrity, coronary anatomy, and biomarker expression in the blood.
The most frequently ordered heart tests in clinical practice fall into four main categories: electrical tests (electrocardiogram, Holter monitor), imaging tests (echocardiogram, cardiac CT, cardiac MRI, nuclear stress test), functional stress tests (exercise stress test, pharmacological stress test), and blood biomarker tests (lipid panel, troponin, BNP). Most patients evaluated for chest pain, palpitations, shortness of breath, or known cardiovascular risk will undergo several of these tests in sequence — each test answering a specific diagnostic question that the others cannot address.
Electrocardiogram (ECG/EKG) — The First-Line Heart Test
The electrocardiogram — abbreviated ECG (from the Greek) or EKG (from the German Elektrokardiogramm) — is the most commonly performed cardiac test worldwide, ordered in virtually every clinical scenario involving potential cardiac symptoms. It takes approximately 5 to 10 minutes to perform, requires no radiation, no needles, and no preparation, and produces immediate results that the ordering provider can interpret within seconds.
The standard 12-lead ECG uses 10 adhesive electrode patches placed on the chest, arms, and legs to record the heart’s electrical activity from 12 different “views” of the cardiac electrical field simultaneously. Each heartbeat produces a characteristic waveform: the P wave (atrial depolarization), the QRS complex (ventricular depolarization and contraction), and the T wave (ventricular repolarization). Deviations from normal waveform morphology, timing, and intervals reveal specific cardiac abnormalities:
- ST elevation in leads corresponding to a coronary artery territory indicates acute ST-elevation myocardial infarction (STEMI) — a medical emergency requiring immediate intervention
- ST depression and T-wave inversions may indicate ischemia, NSTEMI, or electrolyte abnormalities
- Wide QRS complex indicates ventricular conduction delay (left or right bundle branch block) or ventricular tachycardia
- Prolonged QT interval indicates increased risk of life-threatening ventricular arrhythmia (torsades de pointes)
- Left ventricular hypertrophy criteria (increased QRS voltage) indicate long-standing hypertension or hypertrophic cardiomyopathy
- Atrial fibrillation pattern (irregularly irregular rhythm, absent P waves, fine baseline oscillation) is immediately identifiable on ECG
The ECG has important limitations: it captures only 10 seconds of cardiac electrical activity, missing intermittent arrhythmias; it cannot directly assess mechanical function (ejection fraction, valve abnormalities); and a normal ECG does not exclude significant coronary artery disease. For a complete explanation of ECG testing — including how to prepare, what the procedure feels like, and how to interpret your ECG report — see our detailed guide on what is an electrocardiogram.
Echocardiogram — Ultrasound Imaging of the Heart
The echocardiogram (cardiac ultrasound, “echo”) is the primary imaging test for evaluating cardiac structure and mechanical function. Using a handheld ultrasound transducer pressed against the chest wall in several standardized positions, the echocardiogram produces real-time two-dimensional and three-dimensional images of all four heart chambers, all four heart valves, the pericardium (the sac surrounding the heart), and the aortic root.
The key information provided by a standard transthoracic echocardiogram includes:
- Left ventricular ejection fraction — the percentage of blood ejected from the left ventricle with each heartbeat (normal: 55 to 70 percent). The single most important prognostic measurement in cardiology, determining treatment eligibility for heart failure medications, implantable defibrillators, and cardiac resynchronization devices
- Regional wall motion — identifying segments of the ventricular wall that contract poorly or not at all (wall motion abnormalities), indicating either current ischemia or prior myocardial infarction (scar)
- Valve assessment — evaluating all four heart valves for stenosis (narrowing) and regurgitation (leakage), with Doppler velocity measurements quantifying severity
- Pericardial effusion — detecting fluid accumulation around the heart, which if large enough may compress the heart (cardiac tamponade — a life-threatening emergency)
- Diastolic function — assessing how well the left ventricle relaxes and fills (impaired in diastolic heart failure and restrictive cardiomyopathy)
The echocardiogram is painless, uses no radiation, and takes 20 to 45 minutes. For a complete explanation of the echocardiogram procedure, preparation, and findings, see our guide on what is an echocardiogram.
Stress Test — Evaluating the Heart Under Demand
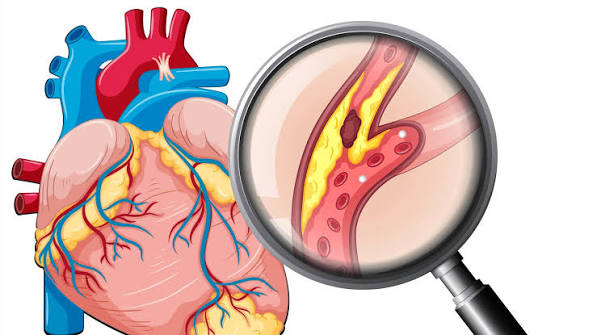
The cardiac stress test is designed to reveal coronary artery disease that is not apparent at rest — because the narrowed arteries of atherosclerosis may supply adequate blood flow to the resting heart muscle but become flow-limiting when cardiac demand increases during exercise. By monitoring the ECG (and optionally, echocardiographic or nuclear imaging of the heart) during standardized exercise or pharmacological stress, the stress test identifies patients with obstructive coronary artery disease, arrhythmias provoked by exercise, or severely impaired cardiac reserve.
The most common form is the exercise stress test (treadmill stress test): the patient walks on a treadmill following the Bruce protocol — increasing speed and incline every 3 minutes — while continuous ECG monitoring, blood pressure measurement, and symptom assessment are performed throughout. A positive test (new ST depression ≥1 mm in two consecutive leads, new ST elevation, or anginal symptoms with hemodynamic compromise) indicates inducible ischemia — typically from a coronary stenosis of 70 percent or greater. The test is terminated when the target heart rate (85 percent of age-predicted maximum) is achieved, or earlier if significant ischemia, arrhythmia, or excessive symptoms develop.
For patients who cannot exercise adequately (due to orthopedic limitations, severe deconditioning, or peripheral artery disease), pharmacological stress testing substitutes medication — adenosine, regadenoson, or dobutamine — to simulate the cardiovascular effects of exercise. Nuclear imaging (SPECT myocardial perfusion imaging) or stress echocardiography is added to pharmacological stress tests because the ECG changes during vasodilator stress are less reliable diagnostically than during exercise.
For a complete guide to the cardiac stress test — including preparation, what to wear, and what results mean — see our detailed article on stress test for heart health.
Cardiac CT Scan — Imaging the Coronary Arteries
Cardiac computed tomography (CT) is the most accurate non-invasive test for visualizing the coronary arteries and quantifying coronary atherosclerosis. Unlike echocardiography (which cannot image the coronary arteries) or standard stress testing (which can only indirectly infer coronary disease from ischemic changes), cardiac CT directly images the coronary arteries with spatial resolution approaching that of invasive coronary angiography.
Two forms of cardiac CT are used in clinical practice:
Coronary artery calcium (CAC) score — a non-contrast CT scan that detects and quantifies calcification within the coronary arteries, expressed as the Agatston score. Coronary calcium is present only in atherosclerotic plaques; its amount correlates strongly with total coronary plaque burden and cardiovascular event risk. A CAC score of zero (no detectable coronary calcium) identifies a very-low-risk group in whom statin therapy and aspirin can often be deferred — the primary clinical use case for CAC scoring is reclassifying patients from intermediate cardiovascular risk to low risk when the CAC score is zero. High CAC scores (above 300 or above the 75th percentile for age and sex) identify patients at very high cardiovascular risk warranting aggressive risk factor management.
CT coronary angiography (CTCA) — a contrast-enhanced cardiac CT that images the coronary arteries during a single breath-hold following intravenous iodine contrast injection. CTCA provides direct visualization of coronary plaque composition (calcified vs. non-calcified vs. mixed) and stenosis severity, with diagnostic accuracy for significant stenosis (≥50 percent) approaching 95 to 97 percent compared to invasive coronary angiography. CTCA is now preferred over stress testing as the first-line investigation for stable chest pain in patients without prior coronary artery disease in major guidelines (ESC 2019, NICE 2016).
For a complete explanation of what happens during a cardiac CT, what radiation dose is involved, and how results are interpreted, see our guide on cardiac CT scan: what it shows.
Blood Tests That Evaluate Heart Health
Blood tests provide biochemical information about cardiovascular risk, myocardial injury, and cardiac function that no imaging test can directly measure. The key cardiac blood tests include:
Lipid panel (fasting): Measures total cholesterol, LDL (low-density lipoprotein — the primary cardiovascular risk driver), HDL (high-density lipoprotein — protective), and triglycerides. Requires 9 to 12 hours of fasting before blood draw. Used to assess cardiovascular risk, guide statin therapy decisions, and monitor response to lipid-lowering treatment. Our articles on LDL vs HDL cholesterol and what is a lipid panel explain the values in detail.
High-sensitivity troponin: The gold-standard biomarker for detecting myocardial injury. Troponin I and T are structural proteins released into the bloodstream when heart muscle cells are damaged or die. Modern high-sensitivity assays can detect troponin elevations within 1 to 3 hours of myocardial infarction onset, enabling the 0-hour/1-hour NSTEMI rule-in/rule-out protocol used in emergency departments. A rising troponin (serial measurements showing >20 percent increase) with at least one value above the upper reference limit diagnoses acute myocardial infarction. Stable mildly elevated troponin may reflect chronic myocardial stress (heart failure, renal failure, pulmonary embolism) rather than acute MI.
BNP and NT-proBNP: B-type natriuretic peptides secreted by cardiac ventricular cells in response to elevated wall stress (from pressure or volume overload). The primary blood test for diagnosing and monitoring heart failure. NT-proBNP above age-adjusted cutoffs (450 pg/mL for age under 50, 900 pg/mL for age 50 to 75, 1800 pg/mL for age over 75) diagnoses acute heart failure with over 90 percent sensitivity in patients presenting with acute dyspnea — helping distinguish cardiac from pulmonary causes of breathlessness in the emergency setting.
Blood glucose and HbA1c: Diabetes is one of the most powerful independent cardiovascular risk factors, doubling myocardial infarction risk. Fasting glucose and HbA1c (glycated hemoglobin — reflecting average blood glucose over the preceding 3 months) are included in comprehensive cardiovascular risk assessment, particularly given the high prevalence of undiagnosed diabetes in patients presenting with cardiovascular disease.
Holter Monitor and Event Recorders — Catching Intermittent Arrhythmias
Because the standard 12-lead ECG records only 10 seconds of cardiac electrical activity, intermittent arrhythmias — atrial fibrillation occurring for a few hours per day, supraventricular tachycardia triggered by specific activities, or ventricular ectopy — are frequently missed on standard ECG. Ambulatory heart rhythm monitors are prescribed to capture arrhythmias during the patient’s normal daily activities.
The Holter monitor is a wearable ECG recorder worn for 24 to 48 hours (or up to 14 days for extended monitoring versions). The patient wears adhesive electrodes connected to a small recording device clipped to their belt or worn as a patch on the chest. The device records continuous ECG throughout the monitoring period. The recorded data is then analyzed by computer algorithm and cardiologist review to identify any arrhythmias, correlating them with the patient’s diary of symptoms and activities.
For palpitations, dizziness, or near-syncope occurring less than weekly (and therefore likely missed even on extended Holter monitoring), implantable cardiac monitors (subcutaneous loop recorders) can be inserted under the skin in a brief outpatient procedure, recording heart rhythm continuously for up to 3 years. Implantable monitors have transformed the diagnosis of intermittent atrial fibrillation in cryptogenic stroke patients — detecting AF in approximately 30 percent of stroke patients within 3 years, compared to less than 5 percent detected by standard 24-hour Holter monitoring.
How to Prepare for Common Heart Tests
Preparation requirements vary by test:
- ECG: No preparation required. Avoid applying lotions or oils to the chest on the day of testing (reduces electrode adhesion).
- Echocardiogram: No fasting or medication changes required. Wear comfortable, easily removed clothing to allow chest electrode placement.
- Exercise stress test: No eating for 3 hours before the test; wear comfortable walking shoes and loose clothing. Your cardiologist will advise whether to hold or continue heart medications before the test (beta-blockers are often held as they blunt the heart rate response).
- Cardiac CT (CTCA): Fasting for 4 hours before contrast injection; heart rate below 65 bpm is required for optimal image quality (beta-blockers may be given before the test); iodine contrast allergy pre-medication if needed.
- Blood tests: Fasting for 9 to 12 hours for lipid panels and glucose. Troponin and BNP do not require fasting.
See our related articles on the annual heart health checkup, what is coronary artery disease, and heart failure symptoms and monitoring. The American Heart Association cardiac tests guide, NHLBI heart tests overview, and ACC/AHA primary prevention guidelines provide additional authoritative information on when heart tests are indicated and what they reveal.
- Agewall S, et al. Expert consensus document on electrocardiographic assessment. Eur Heart J. 2016;37(15):1199-1208.
- Nagueh SF, et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography. J Am Soc Echocardiogr. 2016;29(4):277-314.
- Knuuti J, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407-477.
- Thygesen K, et al. Fourth Universal Definition of Myocardial Infarction. J Am Coll Cardiol. 2018;72(18):2231-2264.
- Grundy SM, et al. 2018 AHA/ACC Guideline on Management of Blood Cholesterol. J Am Coll Cardiol. 2019;73(24):e285-e350.
Cardiac Catheterization and Coronary Angiography — The Definitive Arterial Test
Cardiac catheterization with coronary angiography is the “gold standard” for direct visualization of the coronary arteries — providing the most accurate assessment of coronary stenosis severity and the definitive anatomical guide for decisions about revascularization (angioplasty and stenting, or coronary artery bypass surgery). Unlike all the non-invasive tests described above, cardiac catheterization is an invasive procedure performed in a hospital cardiac catheterization laboratory (cath lab), typically as a day procedure under local anesthesia and intravenous sedation.
During coronary angiography, a thin, flexible tube (catheter) is inserted into a peripheral artery — most commonly the radial artery at the wrist (transradial access, now the preferred approach in most centers due to its lower bleeding risk and shorter recovery compared to the older femoral approach from the groin). The catheter is threaded through the arterial system under continuous X-ray fluoroscopy guidance to the aortic root, where it is positioned at the ostium (opening) of each coronary artery. Iodine-based contrast dye is injected through the catheter into the coronary artery, filling the artery lumen with contrast visible on fluoroscopy — revealing any stenoses (narrowings) as filling defects. The procedure takes 20 to 60 minutes for diagnostic angiography alone.
If a significant coronary stenosis (typically 70 percent or greater diameter reduction) is identified during diagnostic angiography, percutaneous coronary intervention (PCI — balloon angioplasty with coronary stent placement) can often be performed in the same procedure. PCI is the treatment for acute STEMI (performed emergently within 90 minutes of first medical contact — the “door-to-balloon” time target), for significant stable coronary stenosis causing refractory angina, and for high-risk unstable angina or NSTEMI.
Fractional flow reserve (FFR) measurement — using a pressure wire passed through the stenosis during coronary angiography to measure the physiological significance of the stenosis — has become standard in equivocal cases. A stenosis with FFR below 0.80 is hemodynamically significant and benefits from revascularization; FFR above 0.80 (despite apparent angiographic narrowing) can be managed medically, avoiding unnecessary stenting. The landmark FAME and FAME-2 trials demonstrated that FFR-guided PCI reduces adverse cardiovascular events compared to angiography-guided PCI alone.
Cardiac MRI — The Most Detailed Heart Imaging Test
Cardiac magnetic resonance imaging (CMR) is the most comprehensive non-invasive heart imaging test — providing simultaneous assessment of cardiac structure, function, perfusion, viability, and tissue characterization in a single examination, without radiation exposure. CMR is not a first-line test for most common cardiac conditions (the echocardiogram and stress test cover most routine diagnostic needs at lower cost and with greater availability), but it is the reference standard for specific clinical questions where no other test can provide equivalent information:
Myocardial viability assessment: Late gadolinium enhancement (LGE) CMR — performed approximately 10 minutes after intravenous gadolinium contrast injection — identifies non-viable myocardial scar (which retains gadolinium contrast due to disrupted cell membranes) with millimeter-level precision. The transmural extent of gadolinium enhancement predicts whether a myocardial segment that appears akinetic (non-contracting) on echocardiography will recover function after revascularization — guiding decisions about whether coronary bypass surgery will benefit severely impaired ventricular function or merely expose a patient to surgical risk without functional benefit.
Cardiomyopathy differentiation: CMR can distinguish between different types of cardiomyopathy (heart muscle disease) based on the pattern and distribution of LGE — ischemic cardiomyopathy (subendocardial or transmural LGE in a coronary artery territory), dilated cardiomyopathy from myocarditis (mid-wall LGE pattern), hypertrophic cardiomyopathy (patchy LGE at hypertrophied segments), cardiac amyloidosis (global subendocardial LGE with characteristic gadolinium kinetics), and sarcoidosis (septal and patchy LGE with characteristic distribution). These distinctions have direct implications for prognosis and treatment decisions, including implantable defibrillator candidacy.
Congenital heart disease: CMR provides the most comprehensive anatomical assessment of complex congenital cardiac anatomy — including shunt quantification, vessel dimensions, and flow patterns — without radiation, making it the preferred modality for serial monitoring of adults with repaired congenital heart disease.
Nuclear Stress Test (Myocardial Perfusion Imaging) — Mapping Blood Flow to the Heart Muscle
Nuclear stress testing (myocardial perfusion imaging, or MPI) combines cardiac stress (treadmill exercise or pharmacological vasodilation) with intravenous injection of a radioactive tracer (technetium-99m sestamibi or thallium-201) that is taken up by viable, perfused heart muscle in proportion to blood flow. Images acquired at rest and at peak stress are compared to identify areas of reduced perfusion at stress that normalize at rest — indicating viable but ischemic myocardium from obstructive coronary artery disease (reversible perfusion defects). Fixed defects (reduced perfusion both at stress and at rest) indicate non-viable myocardial scar from prior infarction.
Nuclear stress testing provides both diagnostic information (is obstructive coronary artery disease present?) and prognostic information (how much viable myocardium is at risk? Is there evidence of prior infarction?). A normal nuclear perfusion study carries an excellent prognosis — the annual rate of death or myocardial infarction is less than 1 percent per year in patients with a normal nuclear perfusion study, regardless of other risk factors. Large perfusion defects involving multiple coronary territories, especially with associated wall motion abnormalities, indicate severe multivessel disease with high event risk and typically prompt referral for coronary angiography.
The primary limitation of nuclear stress testing is radiation exposure — approximately 10 to 15 mSv for a complete rest-stress study, equivalent to 3 to 5 years of background radiation. This is acceptable for most adults given the diagnostic benefit, but CT coronary angiography (with modern dose-reduction techniques achieving 1 to 3 mSv) has replaced nuclear stress testing as the preferred functional-anatomical imaging test in many centers for appropriate patient populations.
When Are These Tests Ordered — Understanding the Clinical Pathway
Understanding which heart test is ordered and why helps patients navigate cardiac evaluation without confusion or anxiety about what each step means:
Chest pain evaluation in the emergency department follows a well-defined protocol: ECG immediately (to rule out STEMI requiring emergency intervention), serial high-sensitivity troponin at 0 hours and 1 to 3 hours (to rule in or out NSTEMI), and if both are negative in a low-to-intermediate risk patient, either discharge with outpatient stress testing or CT coronary angiography — depending on the risk stratification tool used (HEART score, TIMI score, or GRACE score) and local institutional pathways.
Stable chest pain or exertional dyspnea in a patient with cardiovascular risk factors is typically evaluated with a resting ECG (first), then either exercise stress ECG (if the baseline ECG is normal and the patient can exercise), CT coronary angiography (in guidelines favoring anatomical testing), or stress echocardiography / nuclear perfusion imaging (if the resting ECG has baseline abnormalities that make stress ECG changes uninterpretable, such as left bundle branch block or prior STEMI with Q-waves).
Heart failure evaluation typically starts with ECG (identifying atrial fibrillation, bundle branch block, or prior MI that may explain the failure), BNP or NT-proBNP (confirming the heart failure diagnosis biochemically), chest X-ray (identifying cardiomegaly and pulmonary congestion), and echocardiogram (measuring ejection fraction, identifying the underlying cause — ischemic vs. non-ischemic, systolic vs. diastolic, valve disease, pericardial disease). Coronary angiography or CT coronary angiography follows if the etiology is unclear or if ischemic heart disease is the suspected cause.
Palpitations evaluation starts with resting ECG (if the patient is symptomatic at the time of the ECG, the arrhythmia is immediately captured), then Holter monitoring (24 to 48 hours for daily symptoms), extended event recorder or patch monitor (up to 14 days for weekly symptoms), or implantable cardiac monitor (for monthly or less frequent symptoms, especially after cryptogenic stroke). Echocardiogram is typically performed to exclude structural heart disease that would change the prognostic significance or treatment of any identified arrhythmia.