What Is Basal Cell Carcinoma?
Basal cell carcinoma (BCC) is the most common cancer in humans — more common than all other cancers combined in the United States. Approximately 3.3 million Americans are diagnosed with BCC each year. Despite its extreme prevalence, BCC has the most favorable prognosis of all skin cancers: it almost never metastasizes (less than 0.1% of cases), and when detected and treated at standard sizes, it is curable in the vast majority of patients.
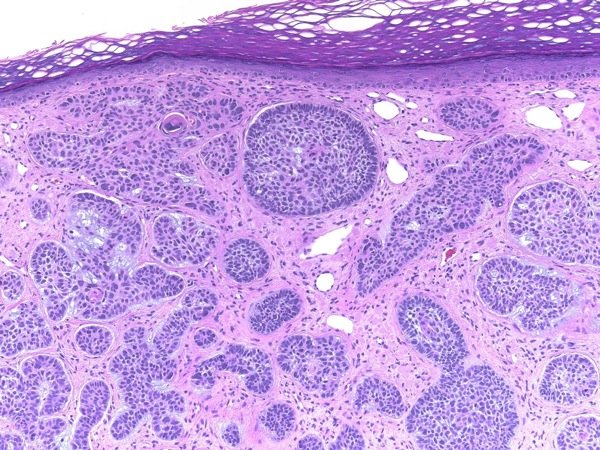
BCC arises from basal cells — the deepest cells in the epidermis that continuously divide to replenish the skin surface. The vast majority of BCCs are driven by cumulative ultraviolet (UV) radiation exposure, which causes mutations in the hedgehog signaling pathway, the molecular circuit that controls basal cell proliferation. When this pathway is constitutively activated, basal cells divide without restraint.
Although BCC does not cause death through metastasis in the way that melanoma or squamous cell carcinoma can, it is locally destructive. Neglected BCCs can invade and destroy underlying cartilage, bone, peripheral nerves, and orbital structures. A BCC on the nose or eyelid that goes untreated for years can cause significant disfigurement and functional compromise. The priority in BCC management is not preventing distant spread — it is achieving complete local eradication before the tumor infiltrates critical structures.
Basal Cell Carcinoma Subtypes
BCC is not a single disease — it includes several clinically and histologically distinct subtypes with different presentations, growth patterns, and treatment implications.
Nodular BCC accounts for 60–80% of all BCCs and represents the “classic” presentation. It appears as a pearly, translucent, dome-shaped papule or nodule, most commonly on the face — particularly the nose, cheeks, and periorbital region. Close examination reveals a rolled, well-defined border and visible surface blood vessels (telangiectasias). In advanced cases, the center ulcerates, producing the classic “rodent ulcer” appearance: a central crater with a raised, pearly border. Nodular BCC grows slowly but predictably, and when caught at small sizes (under 1cm), excision with appropriate margins is curative in nearly all cases.
Superficial BCC presents as a thin, scaly, erythematous plaque, most often on the trunk, shoulders, or extremities rather than the face. It is the least aggressive BCC subtype, growing horizontally along the epidermis rather than deeply into the dermis. Superficial BCC is frequently mistaken for eczema, psoriasis, or tinea, delaying diagnosis. It responds well to both surgical and non-surgical treatments including imiquimod and photodynamic therapy.
Morpheaform (sclerosing) BCC is the most locally aggressive subtype. It presents as an indurated, scar-like, pale or white plaque with ill-defined borders that blend into surrounding skin. Unlike nodular BCC, morpheaform BCC infiltrates well beyond its visible margins — the subclinical extension is frequently substantial, meaning the true tumor edge cannot be determined by visual inspection alone. This subtype has a higher recurrence rate with standard excision and is the primary indication for Mohs micrographic surgery on the face.
Pigmented BCC is a variant of nodular or superficial BCC that contains melanin, giving it a brown, blue, or black appearance that can closely resemble melanoma or a pigmented mole. Dermoscopy reveals arborizing vessels and leaf-like pigment areas — features that distinguish it from melanoma on dermoscopy — but biopsy provides definitive diagnosis.
Basosquamous (metatypical) BCC has histological features of both BCC and squamous cell carcinoma. It is the only BCC subtype with a meaningfully elevated metastatic potential, though this remains low compared to SCC. Basosquamous BCC is treated more aggressively, often with Mohs surgery and close follow-up.
Who Gets Basal Cell Carcinoma: Risk Factors
Cumulative UV exposure is the dominant risk factor for BCC, particularly in fair-skinned individuals with a history of significant occupational or recreational sun exposure. Unlike melanoma (which is more closely associated with intermittent intense sun exposure and sunburns), BCC is linked to cumulative lifetime UV dose.
Skin type: People with Fitzpatrick skin types I and II — fair or very fair skin that burns easily and tans minimally — have the highest lifetime BCC risk. However, BCC can occur in individuals with darker skin tones, typically at lower rates and often without the classic UV-associated histological signature.
Gorlin syndrome (nevoid BCC syndrome): A rare autosomal dominant condition caused by PTCH1 mutations. Affected individuals develop dozens to hundreds of BCCs beginning in adolescence or early adulthood, as well as jaw keratocysts, skeletal anomalies, and falx cerebri calcification. Management includes hedgehog pathway inhibitors (vismodegib) and intensive dermatological surveillance.
Ionizing radiation: Prior radiotherapy to the skin increases BCC risk at the irradiated site, sometimes appearing decades after treatment. This is particularly relevant for patients treated with radiation for head and neck cancers, lymphoma, or acne in earlier medical eras.
Immunosuppression: Organ transplant recipients have significantly elevated BCC risk due to chronic immunosuppression, though BCC risk elevation in transplant recipients is less dramatic than SCC risk elevation.
Arsenic exposure: Chronic arsenic ingestion (historically from contaminated well water or industrial exposure) is a recognized BCC risk factor.

The Hedgehog Pathway: Why BCC Develops
Understanding the molecular basis of BCC is clinically relevant because it directly explains the targeted therapies now available for advanced BCC.
The hedgehog (Hh) signaling pathway normally regulates basal cell proliferation during development and repair. In the resting state, the PTCH1 protein (tumor suppressor) inhibits SMO (Smoothened protein), preventing downstream GLI transcription factors from activating growth genes. UV radiation causes mutations in PTCH1, releasing SMO from inhibition and constitutively activating GLI1 and GLI2 — transcription factors that drive uncontrolled basal cell proliferation.
This mechanism is disrupted in approximately 90% of sporadic BCCs and 100% of Gorlin syndrome BCCs. The SMO protein is the druggable target: vismodegib and sonidegib are SMO antagonists that block this constitutive activation, reducing BCC formation and causing existing BCCs to shrink.
Diagnosis: How BCC Is Confirmed
Experienced dermatologists can diagnose classic nodular BCC clinically with high accuracy. Dermoscopy provides additional diagnostic specificity before biopsy by revealing features characteristic of BCC:
- Arborizing (tree-like) vessels — the most specific dermoscopic feature
- Leaf-like or spoke-wheel pigment areas (in pigmented BCC)
- Blue-gray ovoid nests and globules
- Ulceration or erosion in the center
- Multiple small erosions (superficial BCC)
Histological confirmation by biopsy is required before treatment. A shave biopsy is usually sufficient for nodular and superficial BCC. For suspected morpheaform BCC — where the subtype significantly affects treatment planning — a punch biopsy is preferred to sample deeper dermal tissue and confirm the sclerosing histological pattern.
Surgical Treatment: Excision and Mohs Surgery
Standard surgical excision with appropriate margins is the definitive treatment for most primary BCCs. Recommended margins by risk category:
- Low-risk primary BCC (nodular, superficial; trunk/extremities; <2cm): 4mm margin achieves complete excision in ~95% of cases
- High-risk BCC or recurrent BCC: 5–10mm margins; confirm clear margins on permanent sections
Mohs micrographic surgery is the gold standard treatment for high-risk BCCs, achieving cure rates of approximately 99% for primary BCC and 94% for recurrent BCC. In Mohs surgery, the tumor is removed in sequential horizontal layers; each layer is immediately processed and mapped by the Mohs surgeon, and removal continues only in directions where tumor remains positive. This complete margin evaluation — examining 100% of the surgical margin rather than the sampled margins of standard pathology — allows simultaneous maximal tissue sparing and maximal confidence in complete excision.
Mohs surgery is indicated for:
- BCCs on the “H zone” of the face (nose, nasolabial folds, periorbital area, ear, lips)
- Large BCCs (>2cm on trunk/extremities; >1cm on cheek/forehead/neck; any size on H zone)
- Morpheaform, micronodular, basosquamous, or infiltrative histological subtypes
- Recurrent BCC (previously incompletely excised)
- BCCs with perineural or perivascular invasion
- Immunosuppressed patients
Non-Surgical Treatment Options
For superficial BCC at low-risk anatomical sites — or for patients who cannot undergo or decline surgery — several non-surgical options achieve good clearance rates:
Imiquimod 5% cream: An immune response modifier that activates innate and adaptive immunity to eliminate BCC cells. Applied 5 times per week for 6 weeks, imiquimod achieves histological clearance rates of 80–90% for superficial BCC. Local inflammatory reactions (redness, swelling, ulceration) are expected and indicate treatment response.
5-Fluorouracil (5-FU) cream: A topical chemotherapy agent used for actinic keratoses and superficial BCC. Applied twice daily for 3–6 weeks; effective for superficial BCC at non-critical sites.
Photodynamic therapy (PDT): A photosensitizing agent (aminolevulinic acid, ALA, or methyl aminolevulinate, MAL) is applied to the lesion; after a defined incubation period, the area is illuminated with specific-wavelength red light, generating reactive oxygen species that selectively destroy sensitized tumor cells. Effective for superficial BCC; not recommended for nodular BCC due to inadequate penetration depth.
Curettage and electrodesiccation (C&E): Tumor is scraped out with a curette, then the base is cauterized with an electrosurgical device; repeated in 3 cycles. Effective for small nodular and superficial BCC on non-facial sites. Higher recurrence rate than surgical excision and leaves a circular scar. Not used on morpheaform BCC or high-risk sites.
Advanced BCC: Hedgehog Pathway Inhibitors
For BCC that is locally advanced (cannot be removed with surgery or radiation without unacceptable functional consequences) or, rarely, metastatic, hedgehog pathway inhibitors provide the first approved molecular targeted treatment:
Vismodegib (Erivedge), the first FDA-approved hedgehog inhibitor (2012), demonstrated in the ERIVANCE trial (Sekulic A et al., NEJM 2012) a 30–43% objective response rate in locally advanced and metastatic BCC, respectively — a remarkable result for a cancer that previously had no approved systemic treatment. Side effects include muscle cramps, alopecia, taste disturbance, and fatigue; the drug is teratogenic and requires contraception during treatment.
Sonidegib (Odomzo), FDA-approved in 2015, has a similar mechanism and efficacy profile. The choice between vismodegib and sonidegib is based on tolerability and patient preference.
For Gorlin syndrome patients with high BCC burden, vismodegib significantly reduces new BCC formation and shrinks existing lesions; however, resistance commonly develops, and side effects often limit long-term adherence.
Prevention of Basal Cell Carcinoma
Given BCC’s strong UV dependence, primary prevention centers on minimizing cumulative UV exposure:
- Broad-spectrum SPF 30+ sunscreen applied daily to all sun-exposed skin
- Protective clothing (UPF-rated garments, wide-brimmed hats) during outdoor activities
- Seeking shade between 10am and 4pm when UV intensity is highest
- Avoiding tanning beds
For patients with a history of multiple BCCs, nicotinamide (vitamin B3) 500mg twice daily has demonstrated a 23% reduction in new BCC formation in a Phase 3 randomized controlled trial (Chen AC et al., NEJM 2015). Nicotinamide is inexpensive and well-tolerated, making it a practical chemoprevention option for high-risk patients.
Following any BCC diagnosis, regular dermatological surveillance is essential: patients with one BCC have a substantially elevated lifetime risk of additional BCCs and should have annual to biannual professional skin examinations. See our guide to skin cancer screening for surveillance intervals.
See a dermatologist for evaluation of these BCC warning signs: A pearly or translucent papule on the face that has been slowly growing; a recurring scab or sore on the same spot that heals and then reopens; a flat, scarlike lesion on the face or scalp with indistinct edges; a pigmented lesion on the face or trunk that does not satisfy your expectations of a mole; any new skin growth in a site that has received prior radiotherapy. BCC caught at small sizes is almost always curable with a single procedure. BCC ignored for years may require reconstructive surgery after removal.
Frequently Asked Questions
Is basal cell carcinoma dangerous?
BCC is the most curable form of skin cancer and almost never spreads to other organs. However, “not dangerous” is not the same as “not requiring treatment.” Untreated BCC continues to grow and invades underlying structures. A BCC on the nose or near the eye, if neglected for years, can destroy cartilage or invade the orbit. All diagnosed BCCs require treatment. For a comparison with more dangerous skin cancers, see our articles on squamous cell carcinoma and melanoma.
What is the difference between Mohs surgery and regular excision?
Standard excision removes the BCC with a margin and sends the tissue to a pathologist for next-day margin review. Mohs surgery is performed by a specially trained dermatologist-surgeon who processes and maps the margins in real time during the procedure, allowing same-day confirmation of clear margins. Mohs achieves higher cure rates, spares more normal tissue, and is preferred for high-risk BCCs on the face and other cosmetically or functionally critical areas.
Will my BCC come back?
Recurrence rates depend on the treatment and the BCC subtype. Mohs surgery achieves 5-year recurrence rates of approximately 1% for primary BCC. Standard excision with clear margins achieves recurrence rates of approximately 2–5%. Morpheaform and recurrent BCCs have higher recurrence rates regardless of treatment. Following any BCC excision, continued annual skin surveillance is recommended because the risk of developing additional BCCs is substantially elevated.
Can I develop basal cell carcinoma on my scalp under my hair?
Yes. Scalp BCCs develop in areas of significant UV exposure — particularly in individuals who are bald, have thinning hair, or spend extended time outdoors without head covering. Scalp BCCs are frequently detected late because the area is not easily self-examined and may not be included in routine physician skin checks unless specifically requested. For more information on identifying skin lesions across all body sites, see our guide to skin cancer symptoms.
Sources
- American Cancer Society. What Are Basal and Squamous Cell Skin Cancers?
- National Comprehensive Cancer Network. NCCN Guidelines: Basal Cell Skin Cancer.
- Sekulic A et al. Efficacy and safety of vismodegib in advanced basal-cell carcinoma (ERIVANCE). N Engl J Med. 2012.
- Chen AC et al. A Phase 3 Randomized Trial of Nicotinamide for Skin-Cancer Chemoprevention. N Engl J Med. 2015.
- American Academy of Dermatology. Basal Cell Carcinoma: Overview.
Prognosis and Follow-Up After Basal Cell Carcinoma
Following successful treatment of a primary BCC, the prognosis is excellent. BCC-specific mortality is extremely rare — it is estimated at approximately 0.1% of cases, largely limited to patients with advanced neglected disease, immunosuppression, or the rare basosquamous subtype. The far more clinically relevant concern after treatment is the elevated risk of developing additional BCCs and, to a lesser extent, other skin cancers including squamous cell carcinoma and melanoma.
Published data indicate that patients with a first BCC have approximately a 35–50% risk of developing another BCC within 5 years. This risk is highest in patients who are fair-skinned, have extensive sun damage, or who have already had multiple BCCs. For this reason, dermatological surveillance is not optional after BCC treatment — it is a standard recommendation.
Recommended follow-up after BCC:
- Low-risk primary BCC (first BCC, standard location, completely excised): Annual professional skin examination for life
- High-risk BCC, recurrent BCC, or multiple prior BCCs: Every 6 months for 2–5 years, then annually
- Immunosuppressed patients: Every 3–6 months depending on skin cancer history and degree of immunosuppression
- Gorlin syndrome: Every 3–6 months from adolescence; consider hedgehog inhibitor therapy for high BCC burden
Between professional visits, monthly skin self-examination is recommended. Patients should be familiar with the appearance of their treated BCC site so they can identify local recurrence (which typically presents as a new papule or indurated area at or near the scar edge within the first 2–3 years), as well as new BCCs at other sites. For guidance on screening interval and what professional skin examination involves, see our overview of skin cancer screening.
Basal Cell Carcinoma in Special Populations
Organ transplant recipients: Solid organ transplant recipients have a substantially elevated risk of BCC due to chronic immunosuppression, though BCC risk is elevated to a lesser degree than squamous cell carcinoma risk (which increases up to 250-fold). Transplant recipients should be seen by a dermatologist 6–12 months after transplantation for a baseline skin cancer evaluation and then at intervals determined by their skin cancer history. Any BCC in a transplant recipient should be treated promptly and completely given the impaired immune surveillance that might allow more rapid local extension.
Patients who received radiation therapy: BCC can arise within radiation fields years to decades after treatment. This is particularly relevant for patients who received radiation to the scalp, face, or neck for lymphoma, head and neck cancer, or historically, for acne, ringworm, or other dermatological conditions. These BCCs often appear within the boundary of the treated field and may exhibit morpheaform or otherwise aggressive histological features. Patients with a history of skin radiation should alert their dermatologist so that the relevant skin areas receive focused surveillance.
Young adults with BCC: While BCC is most common in adults over 50, it does occur in younger adults, particularly those with extreme UV exposure history (tanning bed use, outdoor occupational exposure) or genetic predispositions such as Gorlin syndrome. A BCC diagnosed in a person under 40 — particularly if there are multiple lesions — warrants consideration of genetic evaluation for Gorlin syndrome and related conditions. Young patients with BCC often have a long lifetime ahead during which UV exposure will continue to accumulate, making intensive photoprotection and surveillance especially important.
Basal cell carcinoma is a highly manageable diagnosis when recognized early and treated appropriately. The combination of annual dermatological surveillance, consistent sun protection, and prompt evaluation of any new or changing skin lesion allows most patients to manage BCC as a chronic condition without significant morbidity. For a comprehensive overview of how BCC fits into the spectrum of skin cancers — from the most common and curable to the most dangerous — see our guide to skin cancer types and risk factors.
Patients diagnosed with basal cell carcinoma should treat it as a signal about cumulative skin health rather than an isolated event. The same UV damage that produced one BCC is capable of producing additional BCCs, actinic keratoses, squamous cell carcinomas, and potentially melanoma over a lifetime of continued sun exposure. A BCC diagnosis is best understood not as a one-time event to be treated and forgotten, but as a prompt to establish the protective behaviors — rigorous sun protection, monthly self-examination, and regular dermatological surveillance — that reduce the risk of future skin cancers across all types. Identifying and monitoring all concerning lesions through regular professional evaluation remains the most effective long-term strategy for patients with a history of this disease.