Urinary symptoms and the prostate are inseparably linked in men’s health, and the relationship is more complicated than most men realize. Not all urinary changes in men over 50 come from the prostate. Not all prostate problems cause urinary symptoms. And when urinary symptoms prostate cancer does intersect, the relationship is often indirect — involving coexisting BPH more than the cancer itself, particularly in early stages when cancer is most curable.
This guide covers the complete spectrum of urinary symptoms associated with prostate cancer: which ones occur and why, how they differ from BPH, when they signal advanced disease, and what happens to urinary function after treatment. If you’re specifically concerned about frequent urination and prostate cancer, that guide covers the frequency and nocturia aspects in depth.
The Full Spectrum of Urinary Symptoms
The clinical vocabulary for urinary symptoms is organized into three functional categories:
Storage (Irritative) Symptoms
- Frequency: Voiding more than 8 times per 24 hours
- Urgency: A sudden, compelling desire to urinate that is difficult to defer
- Nocturia: Waking from sleep two or more times per night to void
- Urge incontinence: Loss of urine associated with urgency before reaching the toilet
Voiding (Obstructive) Symptoms
- Weak stream: Reduced urine flow rate; peak flow below 10 mL/s on uroflowmetry is clinically significant
- Hesitancy: Delay between attempting to urinate and urine actually starting
- Straining: Need to apply abdominal pressure to initiate or maintain flow
- Intermittency: Flow that stops and starts repeatedly
- Incomplete emptying: Sense of retained urine after voiding
Post-Micturition Symptoms
- Post-void dribbling: Involuntary leakage of urine immediately after voiding
- Feeling of incomplete emptying: The persistent sense that the bladder has not emptied fully
All three categories are grouped under the term lower urinary tract symptoms (LUTS). The presence of LUTS does not identify the cause — BPH, prostate cancer, overactive bladder, infection, or neurological disease can each produce very similar symptom profiles.
Why Early Prostate Cancer Rarely Causes Urinary Symptoms
Approximately 70–80% of prostate cancers originate in the peripheral zone — the outer portion of the prostate that faces the rectum and is palpable on digital rectal exam. The peripheral zone is located away from the urethra, which runs through the center of the prostate within the surrounding transition zone.
Benign prostatic hyperplasia develops in the transition zone — the inner tissue directly encircling the urethra. BPH growth mechanically narrows the urethral channel. Peripheral zone cancer, until it grows large or extends into adjacent structures, has no such mechanical effect on urine flow.
The clinical consequence: approximately 85% of prostate cancers in the United States are found in the localized or regional stage, the majority through PSA testing in asymptomatic men. The cancer is detected by a blood test — not by symptoms — which is why PSA-based prostate cancer screening in asymptomatic men matters. When cancer does produce urinary symptoms, it has progressed locally — grown into the transition zone, invaded the bladder, or produced pelvic metastases.
Storage Symptoms: Frequency, Urgency, and Nocturia
Storage symptoms are the urinary complaints men notice first because they disrupt daily activities and sleep. They are also most commonly attributed to the prostate when the actual cause is often multifactorial.
Urinary frequency and urgency from prostate pathology are most often caused by secondary effects of bladder outlet obstruction on the detrusor muscle. Chronic obstruction causes detrusor overactivity (DO) — this is called overactive bladder (OAB), responsible for urgency and frequency even without direct cancer involvement.
Nocturia in men over 60 commonly reflects nocturnal polyuria (excess urine production at night from age-related hormonal changes), reduced bladder capacity, sleep apnea, and BPH-related obstruction all operating simultaneously. Distinguishing the dominant cause requires a bladder diary and sometimes sleep evaluation.
Voiding Symptoms: Weak Stream, Hesitancy, and Incomplete Emptying
Voiding symptoms — particularly a weak or slow urine stream — are the most specific category for mechanical bladder outlet obstruction. A peak flow rate below 10 mL/s on uroflowmetry suggests significant obstruction and typically prompts cystoscopy to evaluate the outlet directly.
Weak stream from prostate cancer requires that the tumor be large, locally advanced, or located in the transition zone. A standard localized peripheral zone prostate cancer — the type found by PSA screening — does not produce a weak stream. A man who presents with significantly reduced flow and is incidentally found to have prostate cancer on subsequent evaluation almost certainly has his voiding limitation from BPH, not from the cancer itself.
Incomplete emptying, measured objectively by post-void residual (PVR) bladder scan, can cause recurrent UTIs and bladder stones if consistently elevated. PVR above 300 mL is associated with increased complication risk and is an indication for more active BPH treatment.
Hematuria: Blood in Urine and Semen
Of all the urinary symptoms associated with prostate pathology, hematuria — blood in the urine — is the most clinically significant and warrants the most prompt evaluation.
Gross (visible) hematuria is never normal and always requires workup. Microscopic hematuria (blood detected only on urinalysis) also warrants evaluation when persistent. The differential for hematuria in men includes bladder cancer, kidney cancer, urothelial tumors, kidney stones, UTI, and — less commonly — advanced prostate cancer that has invaded the bladder base.
BPH can cause hematuria through engorgement of prostatic vasculature. But when hematuria accompanies elevated PSA, abnormal DRE, pelvic pain, or occurs in a smoker with irritative symptoms, it must not be attributed to BPH without appropriate evaluation including cystoscopy.
Hematospermia (blood in semen) is a separate, highly prostate-specific symptom. In men under 40, isolated hematospermia is usually benign and self-limiting. In men over 50, persistent hematospermia warrants urological evaluation to exclude prostate cancer, particularly with elevated PSA or other risk factors.
When Urinary Symptoms Suggest Advanced Disease
When urinary symptoms are severe, sudden in onset, or accompanied by constitutional symptoms (unexplained weight loss, fatigue, diffuse bone pain), the clinical picture is qualitatively different from routine BPH.
Ureteral obstruction: Locally advanced or metastatic prostate cancer can obstruct the ureters — the tubes draining urine from the kidneys to the bladder. Bilateral obstruction causes hydronephrosis and, if uncorrected, renal failure. Ureteral obstruction from prostate cancer is a urological emergency requiring nephrostomy tube placement or stenting while definitive cancer management is initiated.
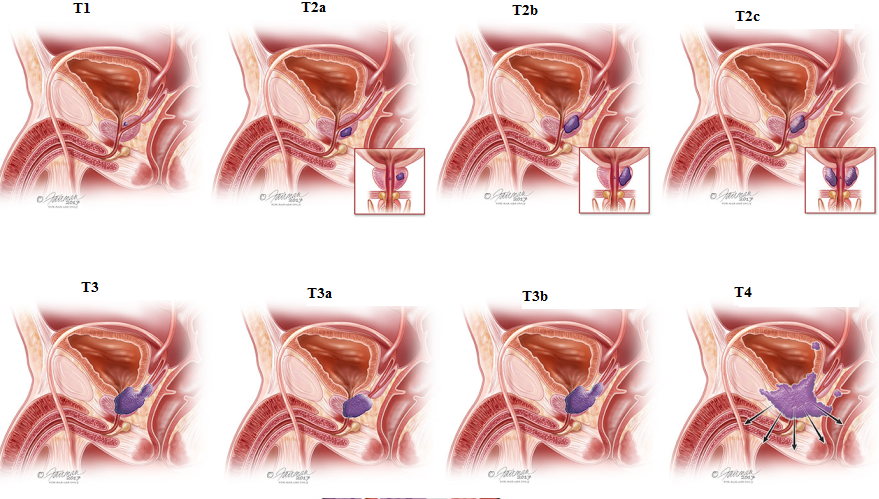
Bladder invasion: Prostate cancer extending through the prostate capsule into the bladder base or neck can directly obstruct the urinary outlet, cause irritative symptoms, and produce hematuria. This is classified as at least T4 (clinical stage) disease.
Neurogenic bladder from spinal cord compression: Metastatic prostate cancer in the vertebral column can compress the spinal cord or cauda equina, disrupting neural pathways that control bladder function. Men may experience urinary retention, incontinence, or loss of the sensation to void. These symptoms with back pain in a man with known prostate cancer constitute a spinal cord compression emergency requiring immediate imaging and treatment.
Urinary Symptoms After Radical Prostatectomy
Radical prostatectomy removes the prostate entirely, which resolves any obstructive BPH symptoms but introduces treatment-related urinary effects men must understand before choosing surgery.
Stress urinary incontinence: The most common post-operative urinary symptom. The external urethral sphincter and pelvic floor bear the primary continence burden once the internal sphincter (at the prostate base) is removed. Immediately after catheter removal, most men experience leakage with physical activity, coughing, or straining.
Recovery trajectory: approximately 20–30% achieve full continence within 3 months; 85–90% are continent by 12 months. Pelvic floor exercises (Kegels) begun before surgery and resumed immediately after catheter removal accelerate recovery. Men with persistent significant incontinence beyond 18 months may benefit from a male sling or artificial urinary sphincter.
Anastomotic stricture: A fibrous narrowing at the urethral anastomosis (surgical connection between urethra and bladder) occurs in 2–8% of cases. It produces a progressively weakening stream, typically appearing 3–12 months post-operatively, identified on uroflowmetry and treated with urethral dilation or endoscopic incision.
Urinary Symptoms After Radiation Therapy
Radiation therapy — both external beam (EBRT) and brachytherapy — affects urinary function through different mechanisms than surgery.
Acute radiation cystitis: During and after EBRT, bladder lining inflammation causes urgency, frequency, and dysuria. Symptoms typically resolve within 4–8 weeks after treatment completion. Anticholinergic medications and increased hydration provide symptomatic relief.
Brachytherapy and urinary retention: Prostate edema from seed implantation causes urethral compression in the weeks following brachytherapy. Urinary retention requiring temporary catheterization occurs in 5–20% of patients, typically resolving as edema subsides over 4–8 weeks.
Late radiation effects: A minority of men develop urethral stricture, radiation cystitis (bladder fibrosis with chronic irritative symptoms), or hemorrhagic cystitis years after treatment. These late effects typically appear 2–5 years post-treatment and may require endoscopic management.
Urinary Symptoms on Hormone Therapy (ADT)
Androgen deprivation therapy (ADT) — achieved through LHRH agonists or antagonists — suppresses testosterone, reducing prostate size. This shrinkage often produces meaningful improvement in obstructive urinary symptoms in men with locally advanced prostate cancer that was compressing the urethra before treatment.
ADT does not typically introduce new urinary symptoms directly. Men on ADT with persistent LUTS are often managed with the same medications used for BPH — alpha blockers and 5-ARIs — though the hormonal context changes the PSA interpretation: a man on ADT has suppressed PSA from both hormone suppression and prostate shrinkage, requiring specific PSA thresholds for monitoring cancer response.
The IPSS in Prostate Cancer Monitoring
The International Prostate Symptom Score (IPSS) is used not only in initial evaluation but also as a monitoring tool throughout prostate cancer management:
- Active surveillance: Serial IPSS scores monitor for symptom changes. A significant IPSS increase during surveillance may reflect cancer progression into the transition zone, BPH progression, or other causes — warranting clinical reassessment.
- After prostatectomy: IPSS tracks continence recovery and identifies men who may benefit from pelvic floor physical therapy or surgical continence procedures.
- After radiation: IPSS monitoring identifies men developing late radiation effects who may benefit from pharmacological or procedural management.
- Visible blood in urine (gross hematuria): Urology evaluation within days
- Blood in semen (hematospermia) in men over 50: Urology evaluation within weeks
- Acute urinary retention (complete inability to void): Emergency room same day
- New or worsening urinary symptoms in a man with known prostate cancer: Contact urologist or oncologist within 24–48 hours
- Lower extremity weakness, numbness, saddle anesthesia with back pain in a man with prostate cancer: Emergency — spinal cord compression
- Fever plus urinary symptoms: Emergency — rule out urosepsis
For a complete picture of all prostate cancer warning signs beyond urinary symptoms, see our guide to prostate cancer symptoms, which covers sexual, bone, and constitutional symptoms. And if you’re navigating what an elevated PSA finding means next, our guide to high PSA evaluation covers each step of the diagnostic pathway.
Frequently Asked Questions
What is the most specific urinary symptom for prostate cancer?
Hematuria — blood in the urine — is the most clinically significant. While not uniquely caused by prostate cancer, its presence alongside elevated PSA, an abnormal DRE, or other risk factors substantially raises concern for malignancy and requires workup. Hematospermia (blood in semen) in men over 50 specifically points toward prostate pathology and warrants evaluation.
Can treating BPH mask prostate cancer symptoms?
BPH treatment does not mask cancer symptoms specifically, because early prostate cancer produces no urinary symptoms. However, 5-alpha reductase inhibitors (finasteride, dutasteride) lower PSA by approximately 50% — which can mask an elevated PSA from cancer if the physician does not double the measured value for cancer screening. Men on 5-ARIs should inform every physician who orders PSA testing about this risk factor context.
Will urinary symptoms improve after prostate cancer surgery?
It depends on what caused them. If pre-operative symptoms were primarily from coexisting BPH, prostatectomy typically improves voiding symptoms. However, it introduces stress urinary incontinence temporarily. By 12–18 months, the majority of men have recovered adequate continence, though timelines vary by age, surgical technique, and baseline continence status.
Do all men with prostate cancer eventually develop urinary problems?
Not necessarily. Men on active surveillance for low-grade cancer may never develop treatment-related urinary changes if they remain on surveillance indefinitely. Men who pursue curative treatment experience treatment-specific urinary effects. The trajectory depends on cancer biology, treatment choice, age, and individual factors.
Sources
- American Cancer Society. Prostate Cancer Signs and Symptoms.
- American Urological Association / Society of Urologic Oncology. Early Detection of Prostate Cancer Guideline (2023 Update).
- National Comprehensive Cancer Network. NCCN Guidelines: Prostate Cancer v1.2024.
- Sanda MG et al. Quality of Life and Satisfaction with Outcome among Prostate-Cancer Survivors. N Engl J Med. 2008;358(12):1250–1261.
- Abrams P et al. The Standardisation of Terminology of Lower Urinary Tract Function. Neurourol Urodyn. 2002;21(2):167–178.
How Bladder Outlet Obstruction Damages the Bladder Over Time
One underappreciated aspect of long-standing urinary obstruction — whether from BPH or locally advanced prostate cancer — is the secondary damage it causes to the bladder muscle itself. The detrusor muscle, designed to contract forcefully and then relax fully, adapts poorly to sustained resistance at the bladder outlet.
In the early phase of obstruction, the detrusor muscle thickens and hypertrophies, compensating by generating higher pressures to push urine through the narrowed outlet. This phase may produce symptoms of urgency and frequency as the overactive detrusor fires prematurely before the bladder is full — the clinical pattern of detrusor overactivity (DO).
In the late phase of obstruction, prolonged against-resistance work causes detrusor decompensation. The muscle becomes thin, trabeculated (with visible bands of fibrous tissue), and loses its contractile strength. At this stage, even if the obstruction is relieved — by TURP for BPH or by cancer treatment — the bladder may not recover full contractile function. Chronic decompensation results in elevated post-void residuals, recurrent UTIs, and sometimes the need for clean intermittent catheterization long-term.
This progression underscores why LUTS in men over 50 warrants clinical evaluation rather than indefinite watchful waiting. A post-void residual that appears minor at first assessment but is allowed to grow over years can cross a threshold where bladder recovery after treatment is incomplete. Early intervention — when the bladder is still compensated — produces better long-term functional outcomes than late intervention after decompensation.
Urinary Symptoms as a Window Into Overall Prostate Health
The pattern of a man’s urinary symptoms over time functions as a longitudinal marker of his overall prostate health — a signal that, when tracked alongside PSA values and DRE findings, creates a more complete clinical picture than any single test or symptom in isolation.
A man with stable LUTS and a PSA that has been flat at 2.5 ng/mL for three years has a different risk profile than a man with the same LUTS score whose PSA has risen from 2.5 to 5.1 ng/mL over the same period. The PSA trend, not the LUTS trend, is what changes the clinical calculus. Conversely, a man with progressively worsening LUTS but consistently normal PSA and benign DRE findings has a very different trajectory — likely representing advancing BPH that needs better medical or surgical management, not a prostate cancer investigation.
Men who track their IPSS scores annually — much as they track blood pressure or cholesterol — build a longitudinal record that is genuinely useful at clinical visits. A primary care physician who can see that a patient’s IPSS rose from 8 to 16 over two years, alongside a PSA rising from 3.0 to 6.2, has far more useful information than one seeing the patient for the first time at IPSS 16. The combination that should always prompt action — worsening LUTS and rising PSA — is more reliably identified when a baseline exists.
For any man over 50 who wants to understand what his urinary symptoms and PSA value mean together, the most productive starting point is a direct conversation with his physician — one informed by an understanding of how prostate cancer risk factors like age, race, and family history interact with these clinical findings to determine how urgently evaluation should proceed.
Differentiating Prostate Cancer Urinary Symptoms from OAB
Overactive bladder (OAB) is frequently misattributed to the prostate in men, and prostate pathology is frequently misattributed to OAB. The clinical overlap is substantial: both produce urgency, frequency, and nocturia. Distinguishing them matters because treatment approaches differ fundamentally.
OAB is defined by urgency — the sudden, compelling desire to void — as the dominant and primary symptom, with frequency and nocturia as consequences. Voiding symptoms (weak stream, hesitancy) are characteristically absent in pure OAB. If a man has severe urgency and frequency but urinates with a strong, fast stream and has minimal post-void residual on bladder scan, his symptoms are more likely OAB than bladder outlet obstruction.
BPH-related LUTS, by contrast, often features a combination of both storage and voiding symptoms — the coexistence of urgency and frequency alongside a weak stream, hesitancy, and elevated post-void residual strongly suggests bladder outlet obstruction with secondary detrusor overactivity.
Prostate cancer in the early, localized setting produces neither storage nor voiding symptoms in most cases. When a man with a prostate cancer diagnosis has prominent storage or voiding symptoms, the most clinically parsimonious explanation is usually coexisting BPH — not the cancer — unless the clinical stage is locally advanced. Understanding this distinction helps men with prostate cancer navigate their symptoms accurately and seek the right interventions.
Tracking urinary symptoms alongside PSA values over time is the most reliable way to distinguish the natural progression of BPH from emerging prostate cancer — and to ensure that neither condition is allowed to advance to a point where treatment options or outcomes are compromised.