DASH Diet for Heart Health
The DASH diet — Dietary Approaches to Stop Hypertension — is unique among heart-healthy dietary patterns because it was specifically designed and validated through rigorous randomized controlled trials for one clear purpose: lowering blood pressure. While the Mediterranean diet emerged from observations of traditional eating patterns and was later tested in clinical trials, DASH was constructed by researchers who identified the nutrients most relevant to blood pressure regulation — potassium, calcium, magnesium, fiber, and sodium — and then built and tested a dietary pattern optimized for those targets.
The result is one of the most clinically validated dietary interventions in cardiovascular medicine. The DASH trial showed blood pressure reductions equivalent to starting antihypertensive medication. When combined with sodium restriction, the DASH-Sodium trial demonstrated the largest blood pressure reduction ever produced by a dietary intervention in a controlled trial. For the approximately 47% of American adults with hypertension — the leading modifiable cardiovascular risk factor — DASH represents a first-line intervention with a level of evidence that few dietary recommendations can match.
What Is the DASH Diet?
DASH was developed and funded by the National Heart, Lung, and Blood Institute (NHLBI) and first published in 1997. Unlike most dietary patterns that develop organically from cultural food traditions, DASH was deliberately constructed: researchers analyzed which nutrients most strongly affected blood pressure based on existing evidence, then designed a dietary pattern that reliably provided those nutrients at levels substantially above typical American intake while restricting the most blood pressure-raising nutrients (primarily sodium and saturated fat).
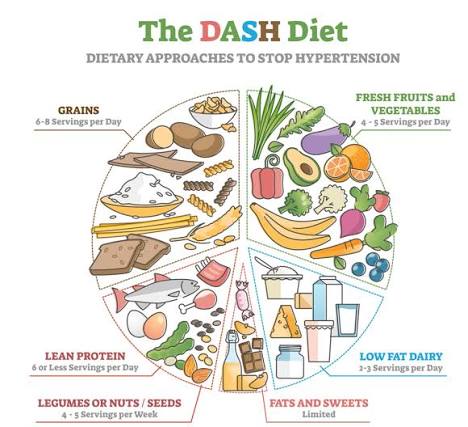
The DASH dietary pattern consists of:
- Vegetables: 4–5 servings per day — the primary sources of potassium and magnesium in the DASH pattern (spinach, sweet potato, broccoli, carrots, tomatoes, leafy greens)
- Fruits: 4–5 servings per day — additional potassium, antioxidants, and fiber (bananas, oranges, berries, apricots, melons, apples)
- Low-fat dairy: 2–3 servings per day — the distinguishing feature of DASH vs. Mediterranean diet; provides highly bioavailable calcium and potassium (skim milk, low-fat yogurt, reduced-fat cheese)
- Whole grains: 6–8 servings per day — fiber, B vitamins, magnesium (oatmeal, brown rice, whole wheat bread, barley, quinoa)
- Lean meats, poultry, fish: ≤6 ounces per day — protein without excess saturated fat; fish counts toward this total
- Nuts, seeds, legumes: 4–5 servings per week — additional potassium, magnesium, plant protein, and fiber
- Fats and oils: 2–3 servings per day — vegetable oils (not butter); total fat kept at approximately 27% of calories
- Sweets and added sugars: ≤5 servings per week — minimized
Sodium targets are explicit and central: the standard DASH diet targets less than 2,300 mg per day — the current Dietary Guidelines limit — while the lower-sodium DASH version targets less than 1,500 mg per day for maximum blood pressure reduction. This sodium target is achievable primarily by reducing processed and restaurant food consumption (which accounts for 71% of dietary sodium) rather than through salt shaker discipline alone.
The DASH Trial and DASH-Sodium Evidence
The original DASH trial enrolled 459 adults with systolic blood pressure between 120 and 159 mmHg and diastolic blood pressure between 80 and 95 mmHg — a range that included people with normal high blood pressure through Stage 1 hypertension. Participants were randomized to one of three controlled eating patterns for 8 weeks: a typical American “control” diet, a diet supplemented with fruits and vegetables only, or the full DASH combination diet. Critically, all food was provided to participants in a controlled feeding design, eliminating adherence as a variable and providing clean evidence for the dietary pattern’s effects under optimal conditions.
The results across arms:
- DASH combination diet vs. control: systolic blood pressure −5.5 mmHg, diastolic −3.0 mmHg (overall population)
- DASH in hypertensive participants (SBP ≥140 or DBP ≥90): systolic −11.4 mmHg, diastolic −5.5 mmHg
- Fruit and vegetables only (no dairy modification): systolic −2.8 mmHg — the full DASH combination was significantly more effective
- Effect was observed within 2 weeks of starting the dietary pattern — faster than most antihypertensive medications reach full effect
A reduction of 11.4 mmHg in systolic blood pressure is clinically equivalent to the effect of a single antihypertensive medication. For patients with Stage 1 hypertension (systolic 130–139 mmHg or diastolic 80–89 mmHg), the 2017 ACC/AHA hypertension guidelines recommend dietary approaches (including DASH) as a first-line intervention before or alongside pharmacological therapy.
The DASH-Sodium trial tested the combination of the DASH dietary pattern with three levels of sodium intake — 3,300 mg/day (typical American), 2,300 mg/day (standard DASH target), and 1,500 mg/day (enhanced reduction) — in a within-person crossover design across 412 adults. Both the DASH diet and sodium reduction independently lowered blood pressure, and their combination at the lowest sodium level produced an 11.5 mmHg systolic reduction — the largest blood pressure reduction ever achieved by a dietary intervention in a randomized trial. Notably, sodium reduction also lowered blood pressure in the control diet group (not just DASH), confirming that sodium restriction is effective even without the full DASH dietary pattern — but that the combination produces the greatest benefit.
How the DASH Diet Lowers Blood Pressure
DASH’s blood pressure benefit operates through five distinct physiological mechanisms, corresponding to the key nutrients the diet is designed to optimize:
Potassium: The DASH diet provides approximately 4,700 mg of potassium per day — the adequate intake established by the National Academies of Sciences and nearly double the US average intake of approximately 2,500 mg per day. Potassium promotes renal sodium excretion by upregulating Na-K-ATPase transporters in the renal collecting duct, directly opposing sodium’s blood pressure-raising mechanism. In vascular smooth muscle, potassium causes hyperpolarization — reducing contractility and promoting vasodilation. Clinical data show that each 1,000 mg increase in daily potassium intake is associated with an average 0.8 to 1 mmHg reduction in systolic blood pressure. The DASH diet’s 4,700 mg potassium target, if achievable from a 2,500 mg baseline, represents approximately 2 to 2.5 mmHg systolic reduction from potassium alone — with the remaining reduction coming from the other mechanisms.
Calcium: The DASH diet targets 1,250 mg of calcium per day, provided primarily by low-fat dairy — the most bioavailable dietary calcium source. Calcium is required for vascular smooth muscle relaxation: after arterial contraction, calcium is actively pumped out of smooth muscle cells to allow relaxation; inadequate dietary calcium impairs this process, contributing to elevated vascular tone and blood pressure. Low-fat dairy (skim milk: 300 mg per cup; low-fat yogurt: 415 mg per cup; reduced-fat cheese: 200 mg per ounce) achieves the DASH calcium target without the saturated fat content of full-fat dairy that would partially offset the cardiovascular benefit.
Magnesium: DASH targets 500 mg of magnesium per day — substantially above the US average of 250 to 350 mg per day. Magnesium acts as a physiological antagonist to calcium in vascular smooth muscle: at adequate concentrations, magnesium occupies calcium channels, reducing calcium influx into smooth muscle cells and promoting vasodilation. Low magnesium status is independently associated with hypertension. The DASH diet provides magnesium through vegetables (spinach, broccoli, beans), whole grains, and nuts — all of which are core components of the pattern for multiple reasons beyond magnesium alone.
Sodium reduction: While not technically a DASH diet nutrient, sodium restriction is an explicit component of the DASH intervention. Since 71% of dietary sodium comes from processed and restaurant foods rather than cooking or table salt, reducing sodium requires reading nutrition labels and reducing processed food consumption — not primarily reducing salt added at the table. The DASH-Sodium trial demonstrated that sodium reduction is independently effective and additive to the DASH dietary pattern for blood pressure reduction, with 1,500 mg/day producing the largest effect.
Fiber: The DASH diet’s 30 grams of daily fiber target improves insulin sensitivity, reducing the compensatory sympathetic nervous system hyperactivity that characterizes insulin-resistant hypertension. Dietary fiber also supports a gut microbiome that produces short-chain fatty acids (acetate, propionate, butyrate) — which have direct vasodilatory effects and reduce systemic inflammation. The fiber contributions come from the full dietary pattern: whole grains, legumes, vegetables, and fruits collectively achieve the 30-gram target that is unachievable without deliberately including these food categories at the recommended frequency.
DASH Diet Food Groups and Daily Targets
Translating the DASH pattern into daily food choices requires understanding what counts as a serving in each category and which specific foods provide the target nutrients most efficiently:
Vegetables (4–5 servings/day): One serving = 1 cup raw leafy vegetables or ½ cup cooked or cut vegetables. Potassium-rich choices: sweet potato (540 mg per medium), white potato with skin (925 mg), cooked spinach (839 mg per cup), cooked broccoli (457 mg per cup), tomato (292 mg per medium). Magnesium-rich choices: cooked spinach, edamame, lima beans. Most vegetables contribute to multiple DASH targets simultaneously — potassium, magnesium, fiber, and antioxidants — making vegetable intake the single highest-leverage DASH action.
Fruits (4–5 servings/day): One serving = 1 medium fruit, ½ cup fresh, or ¼ cup dried. Potassium-rich choices: banana (422 mg), orange (237 mg), cantaloupe (427 mg per cup), apricots (488 mg per 3 dried halves). Berries provide antioxidants and fiber with modest potassium; citrus provides potassium, vitamin C, and folate. The 4 to 5 servings target is achievable by including fruit at breakfast (banana with oatmeal, berries in yogurt), as snacks, and at one meal.
Low-fat dairy (2–3 servings/day): One serving = 1 cup milk or yogurt, 1.5 oz cheese. Preferred: skim or 1% milk, plain low-fat yogurt (Greek or regular), reduced-fat cheese. This is the most distinctive DASH component — the Mediterranean diet does not specifically emphasize dairy, while DASH uses it as a primary calcium source. For lactose-intolerant patients: calcium-fortified unsweetened soy milk (300 mg/cup) and lactose-free dairy provide equivalent calcium.
Whole grains (6–8 servings/day): One serving = 1 slice whole grain bread, ½ cup cooked whole grain (oatmeal, brown rice, barley, bulgur), 1 oz dry cereal (low-sodium). Beta-glucan from oatmeal and barley provides additional LDL-lowering benefit beyond the blood pressure target. Six to eight servings sounds like a lot — it is achievable across meals: oatmeal at breakfast (2 servings), whole grain bread at lunch (2 slices = 2 servings), brown rice or barley at dinner (½ cup = 1 serving), whole grain crackers as a snack.
DASH for Specific Populations
The DASH diet’s blood pressure evidence is strongest overall, but the magnitude of benefit varies significantly by patient characteristics — and certain populations show particularly large responses:
Black Americans: Hypertension is disproportionately prevalent and severe in Black Americans — approximately 55% of Black adults have hypertension, compared to 46% of white adults, with higher rates of early onset, end-organ damage, and related mortality. A key contributing factor is higher rates of salt sensitivity in Black Americans: salt-sensitive individuals show blood pressure increases with sodium intake and decreases with sodium restriction that are 2 to 3 times larger than salt-insensitive individuals. In the original DASH trial, hypertensive Black participants showed a systolic blood pressure reduction of 13.2 mmHg on DASH — larger than the 11.4 mmHg average for the hypertensive subgroup — making DASH particularly impactful for this population. Combined with the high cardiovascular disease burden in Black communities, DASH implementation is a public health priority with documented equity implications.
Older adults: Salt sensitivity increases with age — older adults generally show larger blood pressure responses to both sodium increases and decreases compared to younger adults, likely because of age-related reductions in renal sodium excretion efficiency and vascular compliance. The DASH diet’s blood pressure benefit tends to be larger in adults over 55 than in younger populations in subgroup analyses, making it particularly well-suited as an aging-relevant cardiovascular intervention.
Patients with diabetes or prediabetes: The DASH diet’s high fiber content (30 g/day from vegetables, fruits, legumes, and whole grains), low glycemic load, and magnesium adequacy collectively improve insulin sensitivity — reducing the insulin-resistant hypertension that is particularly prevalent in diabetes and prediabetes. Clinical studies show modest hemoglobin A1c reductions (approximately 0.1 to 0.4%) in diabetic patients following DASH, consistent with the diet’s indirect effects on glucose metabolism through insulin sensitization rather than direct glucose lowering.
Chronic kidney disease patients: The NHLBI specifically recommends DASH for CKD patients with hypertension, as blood pressure control is paramount for slowing CKD progression. For advanced CKD (stage 4 and 5), the potassium content of DASH requires monitoring — hyperkalemia (elevated serum potassium) can occur when renal potassium excretion is impaired. Patients with CKD stage 3b or higher should implement DASH under nephrology guidance, with specific attention to potassium intake from the higher-potassium foods (bananas, white beans, white potatoes, spinach) that may require portion modification in severe CKD.
Practical Implementation and Common Barriers
The most common barriers to DASH adherence in clinical practice — and practical solutions for each:
“I don’t add salt to my food — why is my sodium still high?” The most important insight for patients new to DASH: only 11% of dietary sodium comes from adding salt during cooking or at the table. The remaining 71% is already embedded in processed and restaurant foods before they reach the plate. Effectively reducing sodium requires reading Nutrition Facts labels for sodium content (listed in milligrams per serving) and reducing processed food and restaurant meal frequency — not primarily reducing salt shaker use. Key label reading skill: 5% Daily Value or less (<115 mg) = low sodium; 20% Daily Value or more (>460 mg) = high sodium. For a 1,500 mg/day goal: aim for less than 500 mg sodium per meal from packaged foods.
“DASH is too expensive.” Fresh produce is the most cost-variable component of DASH — but frozen vegetables (broccoli, spinach, peas, edamame, mixed vegetables) and frozen fruits (berries, mango, peaches) are nutritionally equivalent to fresh, frozen within hours of harvest, and cost 40 to 60% less. Canned no-salt-added beans (chickpeas, kidney beans, black beans, cannellini beans) are the most cost-effective DASH food: approximately 50 cents to 1 dollar per can providing 2 to 3 servings of high-potassium, high-fiber, high-plant-protein food. Oatmeal is among the cheapest fiber sources available. A DASH-compatible diet can be achieved on a budget substantially lower than the average American food expenditure.
“I’m lactose intolerant.” The dairy component of DASH can be met through lactose-free alternatives without sacrificing calcium adequacy: lactose-free dairy milk (same nutrients as regular milk, lactase enzyme added), calcium-fortified unsweetened soy milk (300 mg calcium per cup), calcium-fortified orange juice (350 mg per cup), and canned salmon with bones (200 mg per 3-ounce serving) all provide the bioavailable calcium that DASH’s low-fat dairy component is designed to deliver.
“My sodium tastes bland at first.” Salt preference is significantly driven by habit — palates adapted to high sodium find lower-sodium foods bland for the first 2 to 4 weeks of sodium reduction, then re-adapt. Strategies for managing this transition: use fresh herbs, garlic, lemon juice, and spices aggressively as flavor alternatives; add an acid (lemon, lime, vinegar) to dishes — acids interact with taste receptors in ways that reduce the perceived need for salt; use full-flavored ingredients (fresh garlic, onion, fresh herbs rather than dried) to build flavor without sodium. Studies show that sodium preference re-adapts over 4 to 8 weeks of sustained lower-sodium eating, after which high-sodium foods begin tasting excessively salty.
A 7-Day DASH Meal Pattern
A practical weekly pattern consistent with the DASH food group targets and the 2,300 mg sodium limit:
Breakfasts: Steel-cut oats with banana slices, a handful of walnuts, and skim milk (potassium from banana and milk, fiber from oats, calcium from milk); plain low-fat Greek yogurt with berries and 1 tablespoon ground flaxseed (calcium and potassium from yogurt, fiber from flaxseed); 2 eggs scrambled in canola oil with spinach and tomatoes, whole grain toast (potassium from spinach and tomatoes, fiber from toast).
Lunches: Turkey breast (no-added-salt deli turkey or roasted at home) sandwich on whole grain bread with tomato, lettuce, avocado, and mustard (no or low sodium); lentil soup with carrots, celery, and low-sodium broth (potassium from lentils, fiber, plant protein); chickpea salad with cucumber, tomato, red onion, lemon dressing (potassium, fiber, plant protein); canned salmon with no-salt-added crackers and a large vegetable salad.
Dinners: Baked or broiled salmon with roasted sweet potato and steamed broccoli (omega-3s, potassium from sweet potato, potassium and magnesium from broccoli); chicken breast (skinless) with brown rice and green beans, olive oil and garlic; bean and vegetable stew with whole grain bread (high potassium, high fiber); shrimp stir-fry with broccoli, snap peas, bok choy, and brown rice in low-sodium sauce.
Snacks: Banana with 2 tablespoons peanut butter (no-added-salt); low-fat yogurt; apple with a small handful of unsalted almonds; raw carrots and celery with hummus (use low-sodium hummus); orange; unsalted popcorn.
DASH vs. Mediterranean Diet — When to Use Each
Patients and clinicians frequently ask whether to prioritize DASH or the Mediterranean diet. The answer depends on the primary cardiovascular concern:
Choose DASH when: Blood pressure is the primary concern; the patient has documented Stage 1 or Stage 2 hypertension; explicit sodium restriction is clinically indicated; the patient is comfortable with or prefers low-fat dairy as a daily component; the patient wants a structured pattern with explicit serving counts and sodium targets.
Choose Mediterranean when: Overall cardiovascular risk reduction is the primary goal (the PREDIMED trial showed 30% reduction in MI + stroke + CV death — the most direct cardiovascular event evidence of any dietary pattern); the patient has elevated LDL or triglycerides and would benefit from high-EVOO, high-fish omega-3 emphasis; the patient prefers a moderate-fat, higher-flavor Mediterranean cuisine approach; there is no specific clinical sodium restriction requirement.
Either diet (or a combination) is appropriate: For general primary cardiovascular prevention in a patient without specific hypertension or lipid disorders driving the choice; when patient preference and cultural acceptability are the primary driver; when the MIND diet’s combined Mediterranean-DASH approach offers added cognitive benefit alongside cardiovascular protection.
The important point is that both DASH and Mediterranean are evidence-based, both reduce cardiovascular risk through complementary mechanisms, and both share the same positive food foundation — vegetables, fruits, whole grains, legumes, nuts. For patients unwilling or unable to commit to a named dietary pattern, simply increasing intake of these shared food groups while reducing processed food, sodium, and saturated fat moves in the right direction regardless of which label is applied.
Further reading: heart-healthy diet: a practical guide, best foods for heart health, foods to limit for heart health, Mediterranean diet and heart health, and major risk factors for heart disease. Authoritative resources: NHLBI DASH Eating Plan (includes free 30-day meal plan), AHA DASH diet overview, and DASH-Sodium trial (Sacks et al., NEJM 2001).
- Appel LJ, et al. A Clinical Trial of the Effects of Dietary Patterns on Blood Pressure (DASH Trial). N Engl J Med. 1997;336(16):1117-1124.
- Sacks FM, et al. Effects on Blood Pressure of Reduced Dietary Sodium and the DASH Diet (DASH-Sodium). N Engl J Med. 2001;344(1):3-10.
- Chiavaroli L, et al. DASH Dietary Pattern and Cardiometabolic Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses. Nutrients. 2019;11(2):338.
- Lichtenstein AH, et al. 2021 Dietary Guidance to Improve Cardiovascular Health (AHA). Circulation. 2021;144(23):e472-e487.
- National Heart, Lung, and Blood Institute. Your Guide to Lowering Your Blood Pressure with DASH. NIH Publication No. 06-4082. 2006.